A 74 year old patient presented to the emergency room with a syncopal attack. He had an underlying history of untreated adenocarcinoma of the prostate and reported of a 10 to 15 pound weight loss in the recent months.
CBC revealed pancytopenia with white cell count of 0.4 K/uL, hemoglobin of 9.9 g/dl and platelets of 22 K/uL. The clinical suspicion was widespread metastatic adenocarcinoma.
Review of peripheral smear revealed mostly lymphocytes, one blast and a large cell with very granular cytoplasm and large eccentric nucleus.
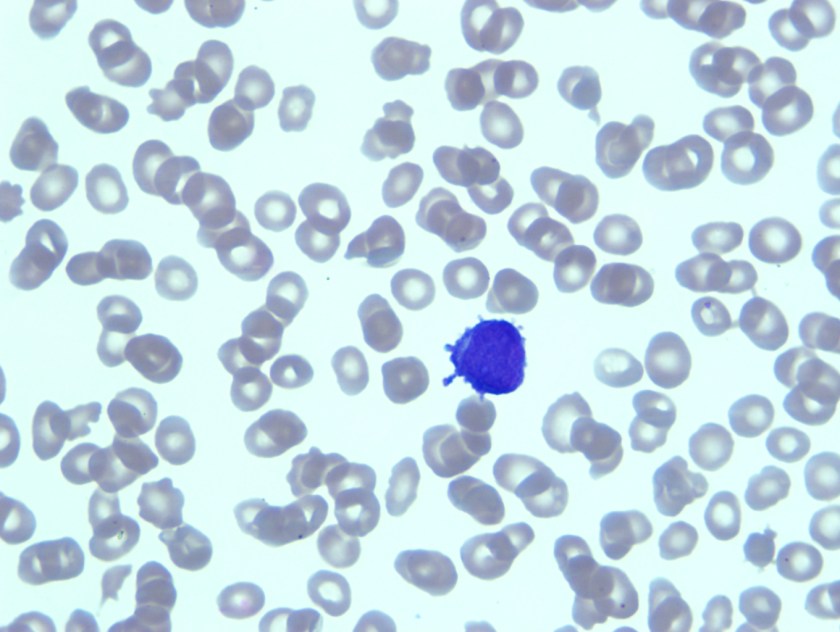
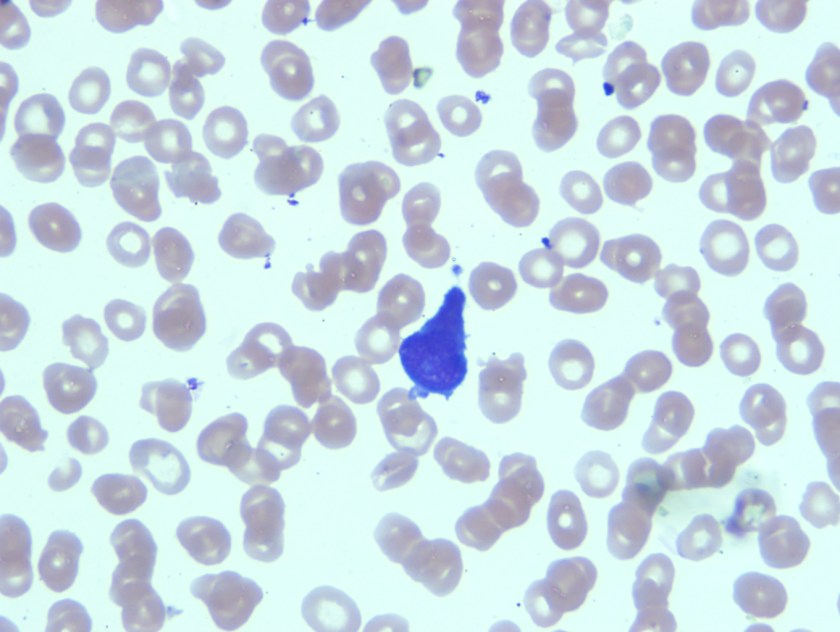
Having reviewed the peripheral smear acute leukemia, likely acute promyelocytic leukemia was considered in the differential diagnosis. As there were no dacrocytes or nucleated red blood cells that were seen on the peripheral smear, it seemed less likely that patient would have metastatic tumor. Bone marrow biopsy was recommended.
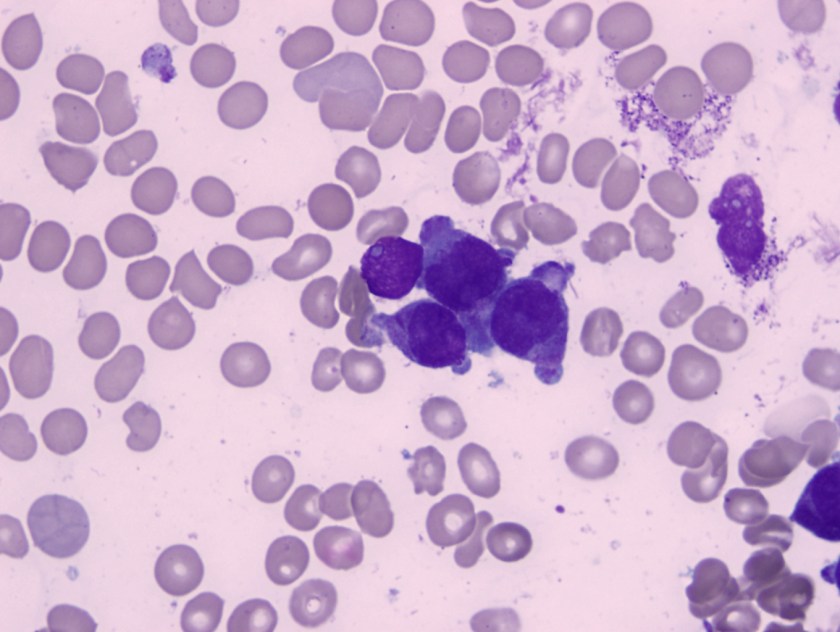
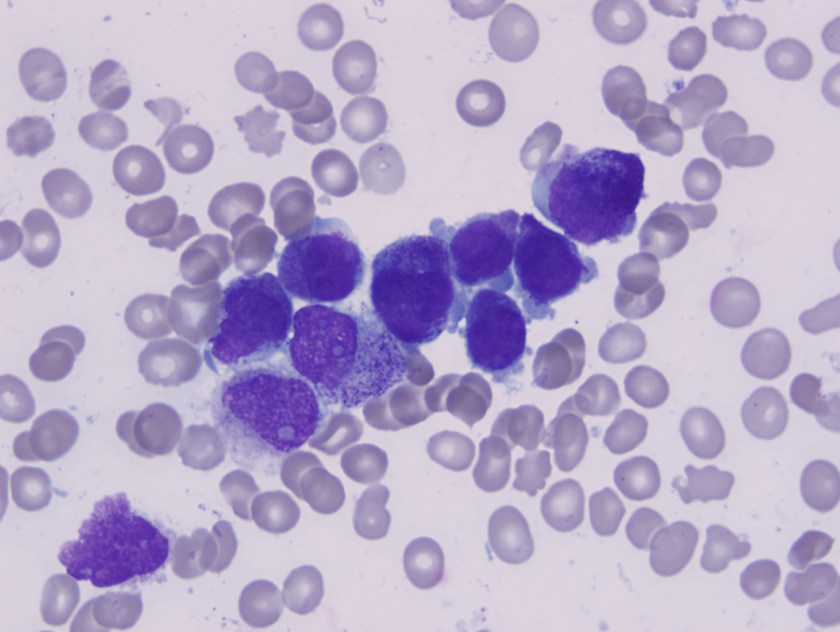
Bone marrow apsirate revealed hypercellular particles with numerous abnormal promyelocytes which were lobulated and hypergranular. Both the karytotype and FISH confirmed the presence of t(15;17).
Acute promyelocytic leukemia with t(15;17)(q22;q12);PML-RARA is an AML in which abnormal promyelocytes predominate. Typical forms are hypergranular (like this patient), although hypogranular (microgranular) forms also exist. Morphological review of the smear is the key to ordering the FISH testing for t(15;17). Often patients with APL present are at increased risk of DIC and needed to be treated on a more emergent basis.
Presence of t(15;17) defines the disease and has a significant therapeutic impact. APL has a particular sensitivity to treatment with ATRA , which acts as a differentiating agent. Prognosis of APL treated with ATRA is much more favorable than other acute myeloid leukemias.

-Neerja Vajpayee, MD, is an Associate Professor of Pathology at the SUNY Upstate Medical University, Syracuse, NY. She enjoys teaching hematology to residents, fellows and laboratory technologists.
