Microaggression is a term first coined by Dr. Chester Pierce, a Harvard psychiatrist, in 1970, where he described the lived experiences of an African American man navigating in white predominant spaces. It took 37 years for the term microaggression to come into mainstream acceptance when it was re-introduced by Dr. Derald Sue in 2007, where he expanded the definition to include general disrespect, devaluation, and the exclusion of minorities.
I still remember my first frozen on-call as a PGY-1 AP/CP resident; I came to work at 6am to prep the gross lab. I was told to fill the big formalin container for the day ahead, log all the refrigerated patient specimens from overnight surgeries, ink to orient and then cut the specimens so they can be fixed. Then finally when I moved to change the water in the stain line, suddenly the tech walked in and asked, “Are you Muslim?” I paused and froze for a moment, didn’t have any words to answer his question. Then I said, “No!”, and he walked away. This incident set me back the whole day, because I was replaying it in my mind again and again, to see why he had asked this specific question to me. Maybe I should have answered differently. I didn’t know of the term, “microaggression” back in 2009.
Now I am equipped with this term and training my colleagues to respond in real-time to these types of instances, I wonder how empowered I would have been if I knew about microaggressions from med school/residency training. I would have been more confident in my interactions, rather than walking on eggshells.
When teaching bystander intervention, there are multiple mnemonics, so that you can quickly react to the situation rather than lack of response in the moment. The 5D’s from American Psychology Association that calls to action are: Distract, Delegate, Document, Delay and Direct. In JAMA Surgery, Dr. Nafisseh Warner introduced GRIT (Gather, Restate, Inquire, Talk It Out). In a learning environment to shift the power dynamics to the clinical learner, the visual below from Dr. Justin Bullock is helpful in breaking down each segment of bystander response: pre-brief, during and after the microaggression.
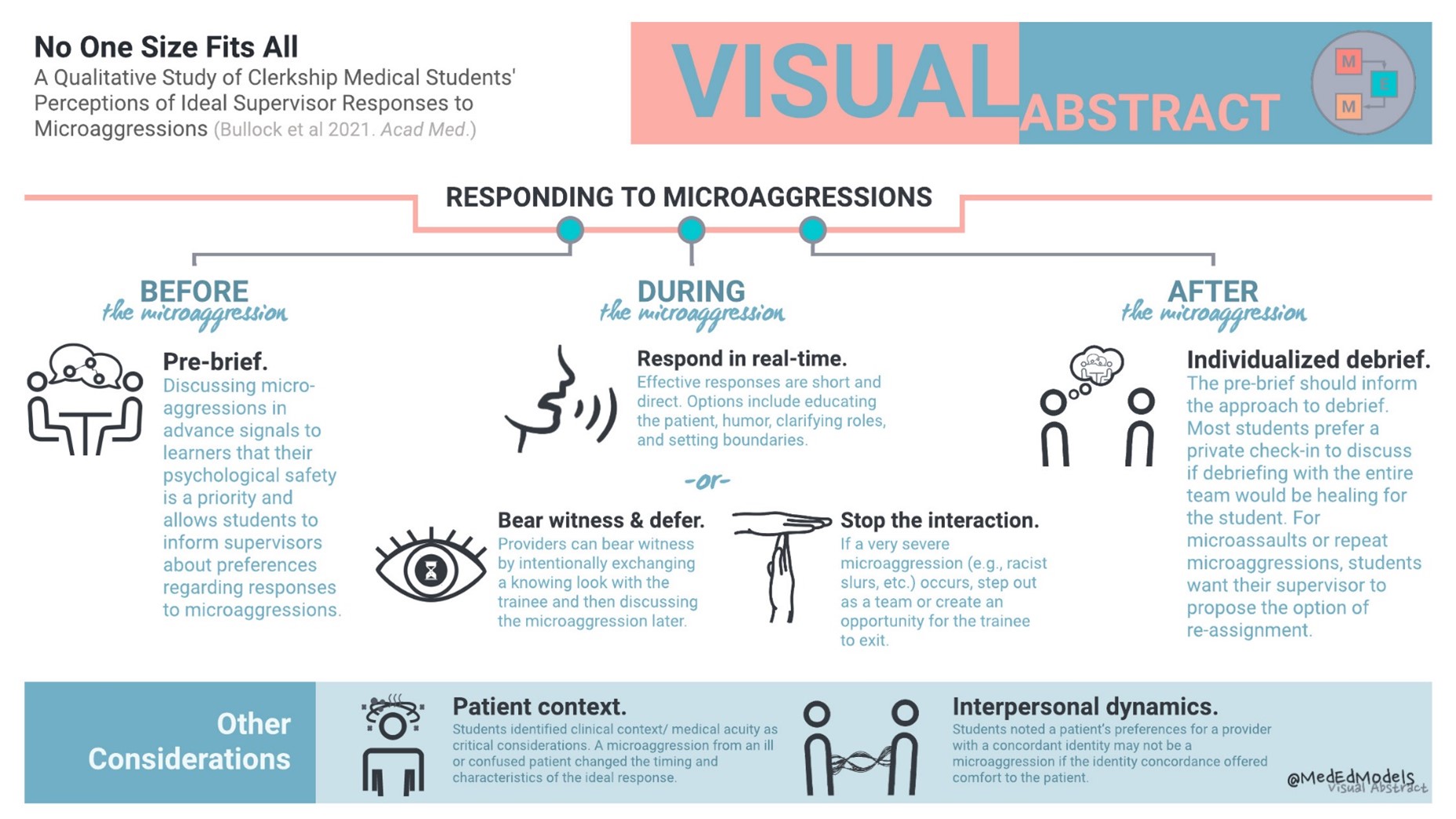
When trainees come into laboratory spaces, it is essential to conduct a pre-briefsession to create a safe-learning environment. During orientation, talk to learners about the possibility of racism and bias. In medicine, the hierarchy is engrained and overemphasized within the system, so learners are hesitant to respond to microaggressions, report bias and racism. Therefore, taking the time to pre-brief will shift the power to learners to say something when being the target of racism and bias.
During microaggression, recognize and analyze it. Is it objectifying? Is it prejudice or negative attitude/stereotype? The usual response to microaggression is no response because you freeze, like I did in my scenario. The effective response is short and direct, most importantly respond in real-time. The degree of response will vary according to the situation and learner’s preference, sometimes the supervisor may bear witness or stop the interaction to create an opportunity for the trainee to exit.
After the microaggression, do not ignore what happened and move on. Supervisors should take the time to privately check-in with the learner and offer support, which is the most preferred approach. Team debriefs might invite an exhausting dialogue and may cause the target to relive the traumatic experience. Also, if there are instances of repeat microaggressions, propose the option for re-assignment.
To create a safe learning environment for our learners it is essential to prioritize psychological safety in our busy clinical services. Taking the time to pre-brief with learners, check-in and offer support to the target will promote a better work culture. Together we can support and empower each other to mitigate microaggressions at our workplaces.

-Deepti Reddi, MD, Assistant Professor of Pathology, Department of Laboratory Medicine and Pathology, UW School of Medicine; UW Medicine’s equity, diversity, and inclusion (EDI) peer trainer at the Office of Healthcare Equity (OHCE) and teaches Racism & Bias for Center for Learning & Innovation in Medical Education (CLIME) in Advanced Clinical Teaching Certificate program. She is also a 2021 ASCP 40 Under Forty Honoree.