Case History
A 62 year old Caucasian male was referred to the gastroenterology clinic with complaints of epigastric pain, diarrhea and unintentional weight loss over the past couple of weeks. Travel history was significant for a recent mission trip to rural areas of the Philippines. During his time there, he participated in building chicken coops and scuba diving. He reported he mostly ate pork & vegetables but did note he consumed a “runny, undercooked duck egg.” He did not eat any seafood during the trip. About a month after his return, he developed epigastric pain and clinically significant diarrhea, with anywhere from 2-8 bowel movements per day. Testing for blood counts, hepatitis and HIV was performed and stool was collected for culture and ova & parasite exam (O&P). He also underwent a colonoscopy with multiple biopsies.


Laboratory Identification
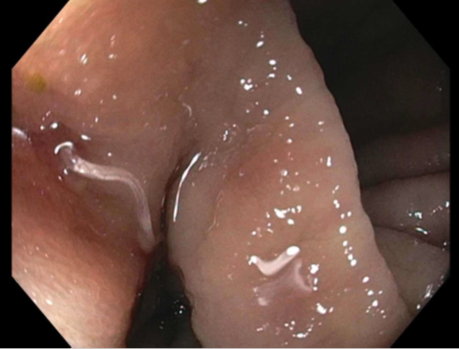
CBC revealed a white blood cell count of 17.9 TH/cm2 with 63.5% eosinophils. Acute hepatitis panel and HIV screen were negative as were two sets of stool cultures and O&Ps. Colonoscopy showed multiple helminths at the ileo-cecal junction (Image 1) and histology of the worms revealed architecture and eggs consistent with Trichuris trichiura (Images 2 & 3).
Discussion
Trichuris trichiura is classified as a nematode (roundworm) and is the third most common round worm causing disease in humans. It has a worldwide distribution and infections are most frequent in areas with tropical climates and resource poor settings with inadequate sanitation practices, especially among children. It is estimated that 800 million people are infected worldwide. While most cases diagnosed in the United States occur in immigrants, travelers and military personnel, T. trichiura has also been documented in the southern United States. Clinical presentations are most frequently asymptomatic or mild. Heavy infections, especially in small children, can cause gastrointestinal problems (abdominal pain, diarrhea, rectal prolapse) and possibly growth retardation due to prolonged malnutrition and anemia.
Infection occurs when embryonated eggs are orally ingested with soil contaminated food & water or due to poor hygiene practices. T. trichiura larvae are released in the small intestine and then travel to the colon where they develop into adult forms. Females begin to produce large volumes of eggs (up to 20,000 per day) about 2-3 months after initial infection. Unembryonated eggs are passed in the stool and in warm, moist soil conditions become infective in 15-30 days.
In the laboratory, diagnosis of T. trichiura is most commonly made by identification of the barrel shaped egg with mucous plugs at either end. The eggs have a double shell and are approximately 50-55 um in length. For increased sensitivity, it is recommended that multiple stool specimens for O&P be collected over the course of 7-10 days as shedding is sporadic. Occasionally, adult worms are visualized on colonoscopy and have a long, thin anterior end which attaches to the mucosa and a thicker posterior portion giving the worm a “whip” like appearance. Adult worms typically measure between 3 to 5 cm in length.
Whipworm infections are routinely treated with albendazole or mebendazole. In the case of our patient, he received multiple doses of albendazole and responded well with resolution of symptoms.

-Joy King, MD, is a fourth year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.

-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. Currently, she oversees testing performed in both the Chemistry and Microbiology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.
